Palatalized implants

The loss of all teeth in a patient’s mouth results in edentulism, which causes:
- Changes in aesthetics: the vertical dimension is lost, altering the facial profile. Lips lose support and appear thinner as their volume decreases.
- A decrease in force and masticatory efficiency (chewing power) occurs following tooth loss.
- Due to the change in the position of the upper jaw (maxilla) and lower jaw (mandible), there is a predisposition for temporomandibular joint (TMJ) issues and muscle-related chewing problems.
- Problems associated with the use of removable complete dentures may arise, such as: stomatitis, angular cheilitis, oral candidiasis, ulcers, and hyperplasia.
Edentulism has significant repercussions on social life and daily activities. Edentulous patients may feel embarrassment when speaking, smiling, or eating in front of others, which can lead to social isolation.
Fill out the contact form if you need to book an appointment at our dental clinic in Valencia
After tooth extraction, the maxillary bone undergoes atrophy. First, there is a loss of bone width in the alveolar process, where the teeth were once anchored. Narrow alveolar processes are classified as Class IV atrophy, where there is sufficient bone height but insufficient width, making it complex to place implants completely surrounded by bone.
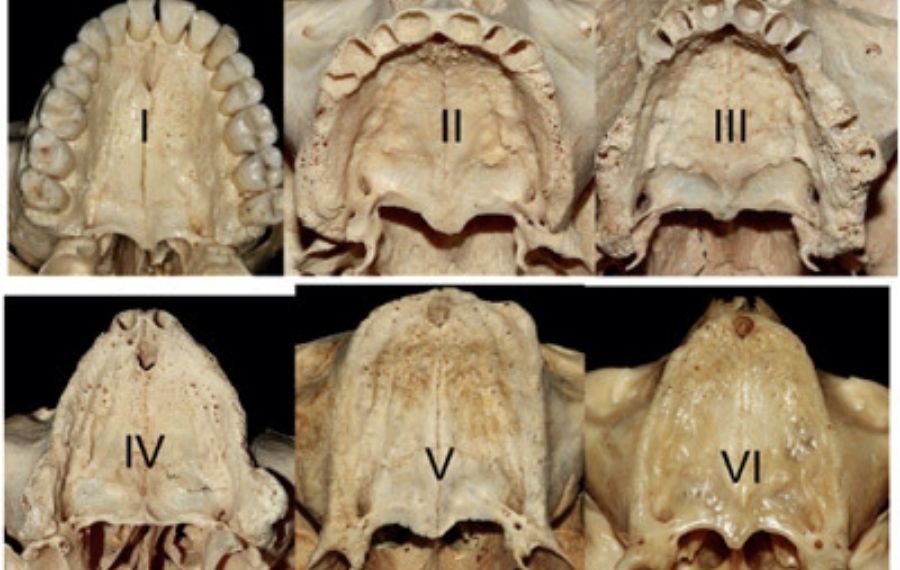
Maxillary bone atrophy is commonly classified according to Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg, 1988; 17: 232-236.
Numerous surgical techniques have been proposed to overcome this situation. Methods for rehabilitating atrophic patients with implants can be classified into bone grafting techniques, such as Guided Bone Regeneration (GBR) or block grafts.
Block grafts are inherently complex to perform. They often result in side effects like swelling and pain, with a 10% to 20% risk of complications—most commonly infection—frequently exacerbated by smoking and poor oral hygiene. Consequently, protocols have evolved to avoid bone grafting by utilizing residual bone areas. These include palatal approach implants, zygomatic implants, pterygoid implants, and angulated implants.
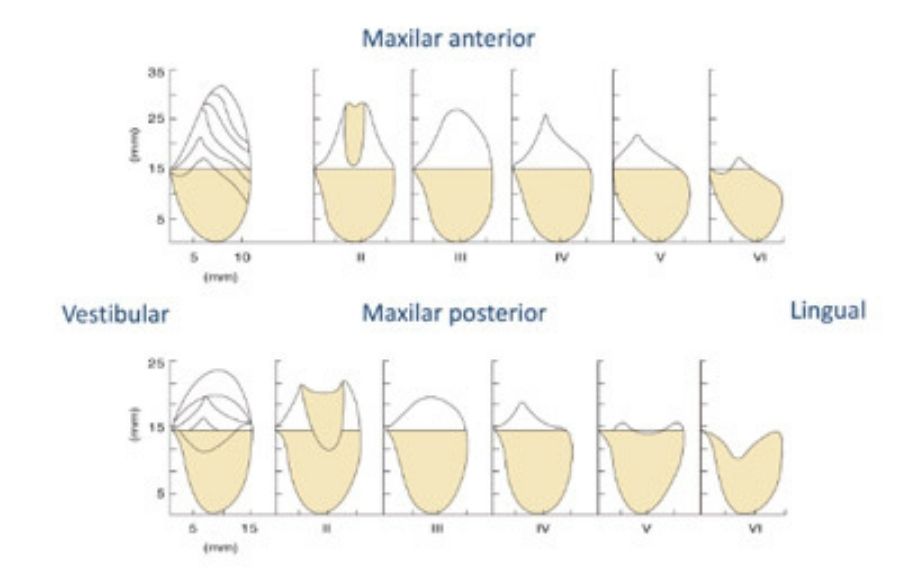
According to Cawood and Howell, the degree of maxillary atrophy is categorized into six grades. Furthermore, based on Bedrossian’s criteria for rehabilitating completely edentulous patients with full-arch prostheses, anchorage is required in at least 2 of the 3 zones (incisors-canines, premolars, and molars), often utilizing cantilevers (with specific limitations).
In cases of complete edentulism with horizontal atrophy of the alveolar process (Class IV atrophic maxilla), there is typically sufficient bone height to place a minimum of 4 to 6 implants distributed across Zones I, II, and III.
Primary stability during implant placement is influenced more by the thickness of the buccal bone than by the length of the implant. Resorption or loss of the buccal cortex can affect peri-implant soft tissue stability and the implant’s survival rate. In Class IV atrophy, palatally placed implants serve as a viable alternative for rehabilitating the atrophic maxilla. These procedures allow us to provide aesthetic and beautiful teeth to patients with significant maxillary atrophy.

The success rate is slightly lower for dental implants placed in grafted bone compared to those placed in native bone. Therefore, whenever we can utilize the patient’s own bone to provide stability, the chances of long-term success increase.
We conducted a study which found that the success rate was slightly lower for dental implants situated in grafted bone compared to those placed in native bone. (Aloy-Prósper A, Peñarrocha-Oltra D, Peñarrocha-Diago MA, Peñarrocha-Diago M. The outcome of intraoral onlay block bone grafts on alveolar ridge augmentations: a systematic review. Med Oral Patol Oral Cir Bucal. 2015 Mar 1;20(2)).
According to the original Brånemark protocol, dental implants should be placed vertically, centered in the bone crest, and completely surrounded by bone; ideally, there should be 2 mm of bone surrounding all parts of the implant.
This position can only be achieved in jaws with sufficient bone height and width (ideally, a minimum width of 8 mm is required, as the implant typically measures 4 mm).
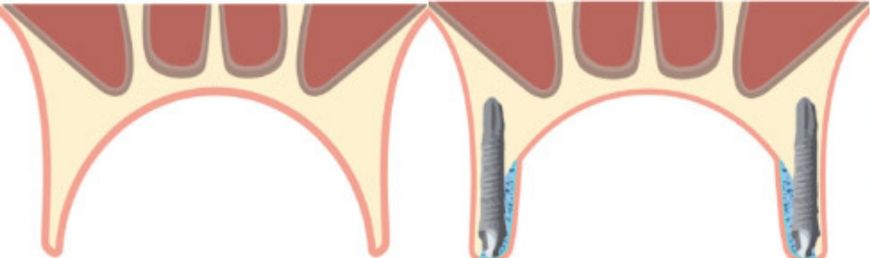
An alternative to bone grafting in jaws with narrow residual crests (under< 4 mm wide) is the insertion of implants in a palatal position. This modification allows for 2 mm of buccal bone even in atrophic crests, while 2 to 5 implant threads are left exposed and covered with particulate bone graft.
The ideal palatal approach implant technique involves: apical anchorage in the palatal cortex, leaving some threads exposed on the palatal side, and subsequently performing simultaneous bone regeneration in that area.
Book an appointment for palatalized implants in Valencia
At the IDIM Institute of Implantology, led by the Peñarrocha doctors, we don’t just care for your smile—we provide effective solutions, backed by our extensive experience and dedication.
With over 30 years of specialization in dental implantology, we apply advanced techniques and cutting-edge technology to ensure the best results for our patients.
Fill out the following form and book an appointment for your palatalized implants treatment in Valencia with no obligation.



+34 963 34 46 75